
Please note: this is the fifth of a 5-part blog. (see Parts 1, 2, 3 & 4)
Dorsal Vagal or Parasympathetic Nervous System • Collapse
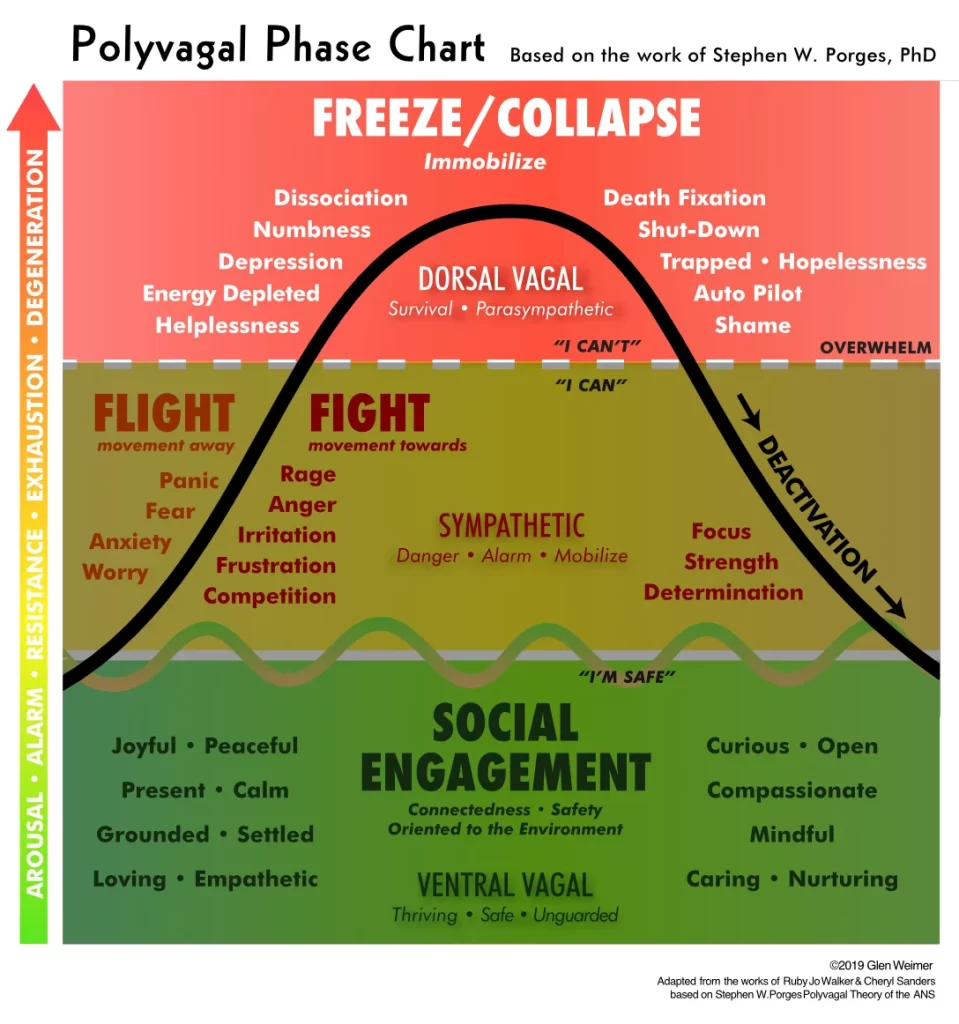
In Part 5 we will examine the Dorsal Vagal Complex (DVC)/Parasympathetic Nervous System (PNS): how it immobilizes our BodyMind System (BMS) to freeze or collapse when facing life-threatening situations, its role in childhood development, as well as healthy and unhealthy expressions. Like the Sympathetic NS it is neither inherently good or bad. It’s our RED LIGHT / Full Stop Mode!
Unlike with Sympathetic NS activation, where our response to threats mobilizes us to fight or flee / confront or avoid, we engage our Dorsal Vagal when we perceive life-threatening danger that is extreme and overwhelming. It is more than the BMS can handle in the moment so we shut down, dissociate and prepare for death. This level of overwhelm induces persistent trauma patterns in the BodyMind System, which are, in fact, the system’s own reminders of where to focus on healing when the danger has passed.
On the other hand, with no perception of threat, the combined Ventral Vagal and Dorsal Vagal branches of our Parasympathetic Nervous System work together, enabling us to sit still, go inward, and calm our internal world. DVC draws our energy, blood supply, and consciousness away from the periphery of our bodies back into the vital organs to maintain core body functions and sustain life.
Childhood DVC Conditioning
 In part 4 of this blog, we talked about how childhood is designed to teach us to co-regulate and fluidly shift between Sympathetic activation and Ventral Vagal safety. Unfortunately, often there were moments in childhood or the entirety of our formative years, where we did not have a safe container to develop this skill or to associate mobilization with fun. We may have been teased, shamed, bullied, or even abused, where the impulse to fight or run was not a viable option. Others were much bigger, stronger, older, and we were simply not able to avoid a bad outcome; activation didn’t happen within a safe context. Sometimes it’s a response to something ‘bad’ happening—we got hit and couldn’t defend ourselves, other times it’s in response to something ‘good’ not happening—we REALLY needed a hug in that moment, but no one was there to comfort and reassure us. Instead of mobilizing our SNS to defend ourself we dropped into our Dorsal Vagal (DVC) and ‘disappeared’; dissociating or retreating to a deep inner refuge.
In part 4 of this blog, we talked about how childhood is designed to teach us to co-regulate and fluidly shift between Sympathetic activation and Ventral Vagal safety. Unfortunately, often there were moments in childhood or the entirety of our formative years, where we did not have a safe container to develop this skill or to associate mobilization with fun. We may have been teased, shamed, bullied, or even abused, where the impulse to fight or run was not a viable option. Others were much bigger, stronger, older, and we were simply not able to avoid a bad outcome; activation didn’t happen within a safe context. Sometimes it’s a response to something ‘bad’ happening—we got hit and couldn’t defend ourselves, other times it’s in response to something ‘good’ not happening—we REALLY needed a hug in that moment, but no one was there to comfort and reassure us. Instead of mobilizing our SNS to defend ourself we dropped into our Dorsal Vagal (DVC) and ‘disappeared’; dissociating or retreating to a deep inner refuge.
Conversely, the safer we felt to engage with our outer world during childhood, the more Resources we developed both to shift out of Sympathetic activation back to Ventral Vagal social engagement; as well as to shift between DVC and VVC, recovering more easily from traumatic events to return to feeling calm, at peace and secure in the world. (see my blogs on Resourcing and Overwhelm).
Longterm DVC Shutdown
 The more individual and extended traumatic events we’ve experienced in life; the less Resources we have to draw upon to return to a healthy homeostasis. Trauma survivors without self- or co-regulatory skills can find that even small moments of distress feel draining and unbearable. The system immediately freezes or collapses rather than mobilizing in any way. If you’ve ever just wanted to close out the world and curl up into a fetal position, you know this state.
The more individual and extended traumatic events we’ve experienced in life; the less Resources we have to draw upon to return to a healthy homeostasis. Trauma survivors without self- or co-regulatory skills can find that even small moments of distress feel draining and unbearable. The system immediately freezes or collapses rather than mobilizing in any way. If you’ve ever just wanted to close out the world and curl up into a fetal position, you know this state.
We end up feeling disconnected from our body, our life and our world. Ongoing physical and psycho-emotional pain causes us to ‘abandon ship’, removing our consciousness from those areas or from our bodies entirely. We isolate and distance ourselves from family and friends because social interactions have the potential of danger. We can feel alone, lost, like we can’t find our way back, often even fixated on death as an escape when the ‘fight’ is just too hard.
 In DVC, our neuroception determines that there is no action that can change a negative outcome or situation, and its last resort is to deflate and crumble. The perception is of imminent DEATH! Often people will actually say, “Oh my God, I feel like I’m going to die!”
In DVC, our neuroception determines that there is no action that can change a negative outcome or situation, and its last resort is to deflate and crumble. The perception is of imminent DEATH! Often people will actually say, “Oh my God, I feel like I’m going to die!”
These can be isolated life events from any point in our past: like falling as an infant, being fired from a job, a car accident, robbery, or the unexpected death of a loved one. They can also be periods of time that were overwhelming to us: like being molested or bullied throughout childhood, or being in an abusive marriage. But we can even experience less dramatic events as overwhelming. It is the perception rather than the event that is important! For example: it’s 4:45pm, we have a huge stack of work to get done and the boss puts one more thing on the pile to be completed before we leave. Internally, that small incident can feel immense and catastrophic.
Typically, we blame ourselves for not acting or we judge ourselves through others’ eyes for how we imagine they perceive us. What we fail to recognize or fully appreciate is that our Dorsal Vagal response is an autonomic, automatic, subconscious whole body reaction to a perceived life-threat. It all happens before and without any conscious awareness or control. IT IS what kept us alive, physically and/or psycho-emotionally. The first step in returning to autonomic homeostasis is to acknowledge our system’s extraordinary wisdom in mustering this global response to save our life.
The BodyMind’s Response
The common denominator is a feeling of utter disempowerment. The body’s response is to prepare for death. We anesthetize or numb ourselves so we don’t feel the pain as acutely, and we dissociate from our body so we’re ‘not there’ when extreme pain, humiliation, or death comes. Our nervous system takes control and immobilizes our muscles so we can’t run or fight (even if we want to). In extreme cases of sudden fright, we may get lightheaded, faint, or go unconscious and even lose control of our bladder and bowels.
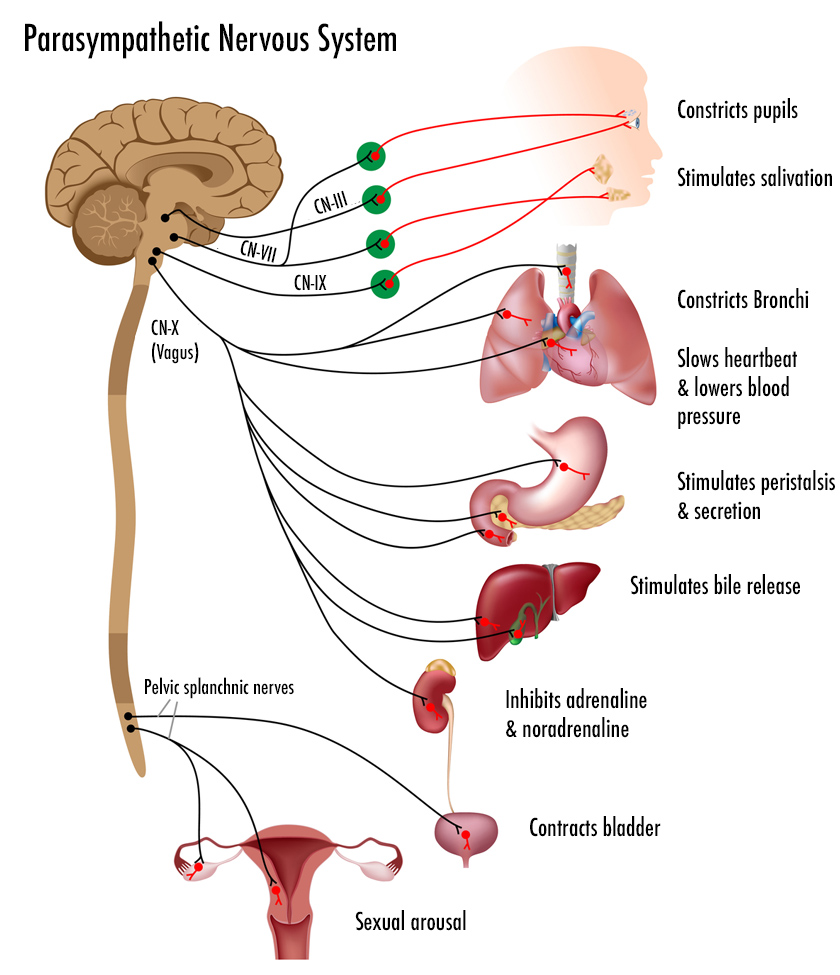 Physiologically, it’s like we turn all the dials down to low, conserving our life-energy. Our body is functioning at a baseline, survival level. Our heart rate slows and bronchi of the lungs constrict. Our metabolism also slows. We can often feel sleepy, drained, lethargic, unmotivated, barely alive. We feel both helpless and hopeless.
Physiologically, it’s like we turn all the dials down to low, conserving our life-energy. Our body is functioning at a baseline, survival level. Our heart rate slows and bronchi of the lungs constrict. Our metabolism also slows. We can often feel sleepy, drained, lethargic, unmotivated, barely alive. We feel both helpless and hopeless.
For reptiles the freeze response is a way to appear inanimate and invisible so the threat will pass by. This same response in humans consumes a great deal of energy to maintain immobilization in the face of a possible death. Like a deer in headlights, this freeze locks down the sympathetic impulse to act, making the gas-petal/break response a chronic underlying state.
In dysregulated DVC our facial affect and voice are flat, emotionless and disconnected from the world. Our face can lose its color and appear lifeless and unresponsive. Our eyes may have a vacant, distant stare. Our muscles and connective tissues lose their normal tone and can seem flaccid/slack. Our body feels too heavy to support.
In his book “Accessing the Healing Power of the Vagus Nerve”, Stanley Rosenberg states, “Even small tasks seem to take monumental effort. Our heartbeat slows and our blood pressure drops; the blood withdraws from the periphery of the body and gathers in the center. Our hands and feet feel cold and clammy. When we are in a dorsal vagal state, we often have pains that move around to different parts of the body…”
The Digestive System
When both branches of our Vagus Nerve pathways (VVC and DVC) work together, our digestive system functions optimally, as described in part 3; we are in Rest, Digest, and Rebuild mode. Our mouth secretes saliva to begin breaking down food; the stomach produces acid; and the liver and pancreas release enzymes into the small intestine to complete the digestive process. Increased intestinal motility moves this along, assimilates the nutrients and eliminates waste. On the other hand, a dysregulated DVC can lead to irritable bowel syndrome, bloating, heartburn, diarrhea, and other digestive issues.
In a session, when my clients release frustrated Sympathetic tension from their bodies, the first thing I notice is Borborygmus (tummy rumbling). As their full PNS kicks in, digestive juices are secreted and intestinal peristalsis re-engages.
Breath & Pulse
In DVC, like in SNS, the breath can be held in a frozen inhalation. In SNS, it’s held by a frustrated activation response, while in DVC, it can get locked down by a sudden shock eliciting a sharp inhale (freeze). Conversely, it can also be as if we’ve had the wind knocked out of us and we can’t get a full in-breath (collapse). These should be considered as two distinct responses: Freeze, often to an abrupt, unexpected situation (shock-response); and Collapse, to long-term depletion of the system’s ability to defend itself. In either case, the Dorsal Vagal Complex can constrict the air passages, leading to extreme breathing dysfunctions.
 With a frustrated Sympathetic NS, returning to Ventral Vagal co-regulation requires down-regulating an overstimulated system through slowing down the breath and focusing on an extended exhalation. By contrast, in order to assist an overwhelmed DVC in returning to balanced homeostasis, we need to increase our cardio with full deep breaths, driving oxygen into the body, blood flow into the tissues, and up-regulating the nervous system. In essence we have to pass back through our SNS to reach Ventral Vagal co-regulation. (see the exercise at the end of this blog.)
With a frustrated Sympathetic NS, returning to Ventral Vagal co-regulation requires down-regulating an overstimulated system through slowing down the breath and focusing on an extended exhalation. By contrast, in order to assist an overwhelmed DVC in returning to balanced homeostasis, we need to increase our cardio with full deep breaths, driving oxygen into the body, blood flow into the tissues, and up-regulating the nervous system. In essence we have to pass back through our SNS to reach Ventral Vagal co-regulation. (see the exercise at the end of this blog.)
The challenge is that, in reengaging the Sympathetics we wake up what I call ‘the ugly awfuls’, all those unpleasant sensations, emotions and memories that our down-regulated nervous system enabled us to suppress or avoid. Addiction, particularly substance abuse, is one way of maintaining Dorsal Vagal Freeze/Collapse so we don’t have to re-experience all that. Alternatively, we might use TV, video games, books, movies, sleep or any number of other ways to escape the challenges of our lives. Each time we try to recover by bringing more awareness to the issues and begin to run more energy through our bodies we may feel anxious, shaky, angry as the ugly awfuls resurface. So we ‘self-medicate’ to drop back into our familiar low-energy state of numbness.
It is critical in Dorsal Vagal trauma recovery to have adequate support, both from experienced professionals and family/community, to ensure that we don’t re-traumatize ourselves in the healing process. Fortunately, there are highly skilled verbal counselors in every community and many emerging non-relive body-centered (somatic) trauma techniques to support healing overwhelm.
DVC In Health
Having both VVC and DVC branches working in harmony, enables us to settle our nervous system, to meditate, concentrate, and seamlessly shift between our inner and outer worlds. It truly is our rest and rebuild state. Our vital organs function optimally, and energy/consciousness is directed back into our core to repair damaged tissues, remove waste and recharge our mental/emotional and physical batteries. Our digestive system is secreting fluids to facilitate digestion, assimilation and excretion; our heart and lungs are maintaining a slow steady effortless rhythm; our lymphatic and immune systems are busy with tissue repair and waste removal; and our endocrine system is orchestrating homeostasis.
 The key to a resilient, integrated Autonomic NS with all three branches co-regulating and functioning optimally is Resourcing, drawing on our webwork of interconnections to meet life’s challenges. Ventral Vagal Interpersonal Resources connect us to the support of our outer world: friends, family, community, etc. Sympathetic Intra-personal Resources connect us to all the parts of our self working seamlessly in concert: mentally, emotionally and physically (like a peak-performance athlete). Dorsal Vagal Transpersonal Resources connect us to the ‘Divine’: God, the Universe, Nature, creativity, etc. (see Resourcing)
The key to a resilient, integrated Autonomic NS with all three branches co-regulating and functioning optimally is Resourcing, drawing on our webwork of interconnections to meet life’s challenges. Ventral Vagal Interpersonal Resources connect us to the support of our outer world: friends, family, community, etc. Sympathetic Intra-personal Resources connect us to all the parts of our self working seamlessly in concert: mentally, emotionally and physically (like a peak-performance athlete). Dorsal Vagal Transpersonal Resources connect us to the ‘Divine’: God, the Universe, Nature, creativity, etc. (see Resourcing)
A co-regulated VVC and DVC not only allows us to settle and slow our breathing and pulse, but it enables us to enter meditative and expanded states of consciousness where we can have direct experiences of the Divine. But we even reach for that transpersonal connection as our last hope when all else fails. As we move into dysregulated DVC, in desperation, we often repeat the mantra, “God, please help me!”. Additionally, when we retreat internally or dissociate, we connect to our personal inner spirituality and/or to creative outlets to channel our distress.
DVC In Therapy
In cases of frustrated Sympathetic Fight or Flight, a person’s muscles, organs and other tissues are locked in a perpetual contractive, hypertensive state. Energetically, the forces of consciousness are centripetally drawing inward, from the periphery to the center. Here, therapeutically, we are helping the tissues to feel safe enough let go and relax. (see part 4)
By contrast, when a person (that’s all of us), has experienced DVC overwhelm, the tissues in the associated area of the body feel ‘blown-out’, they lack elasticity, vitality, integrity—they just feel dead! They have little or no rhythmic motility, not because they’re holding as with SNS, but because there’s ‘nobody home’. Just as with the psycho-emotional level, here body-consciousness within the tissue field has moved out to the periphery of the field (centrifugally) and never came back. The energy or consciousness has dissociated from the body.
 When I work on these parts of the body, I first need to make it safe for the client to bring awareness back into the body. I may do this by simply holding that area, without asking anything from it; I show up with a still, loving presence. Remember, this tissue is the byproduct of the perception of an extreme life-threat. I bring the same presence I would when cradling a wounded bird or baby, and I wait for some small piece of body-conscious to show up and meet me. Then I may initiate a slow, subtle pulsing with my hands; lightly encouraging the tissue field to come back to life. It’s like doing energy-CPR in one small area of the body. Once the tissues begin to move even slightly, I can move one hand away to make contact with neighboring areas, creating a Polarity relationship that reminds the parts they are components of an interconnected whole.
When I work on these parts of the body, I first need to make it safe for the client to bring awareness back into the body. I may do this by simply holding that area, without asking anything from it; I show up with a still, loving presence. Remember, this tissue is the byproduct of the perception of an extreme life-threat. I bring the same presence I would when cradling a wounded bird or baby, and I wait for some small piece of body-conscious to show up and meet me. Then I may initiate a slow, subtle pulsing with my hands; lightly encouraging the tissue field to come back to life. It’s like doing energy-CPR in one small area of the body. Once the tissues begin to move even slightly, I can move one hand away to make contact with neighboring areas, creating a Polarity relationship that reminds the parts they are components of an interconnected whole.
Additionally, I may utilize verbal body-centered trauma techniques, where we do much the same thing through dialogue. I’ll start out by assisting the client to find or create a sense of internal safety. Safety is always primary! Ventral Vagal co-regulation is what was lacking, which created this internal distress, so it must be re-established for healing to occur. I then may draw the client’s awareness to areas of pain or discomfort in their body and help them to dissipate those sensations through Resourcing that part to other ‘good-feeling’ areas; or to pleasant memories, emotions, or uplifting thoughts and images. The dialogue brings the client’s awareness to how their thoughts, feelings and memories live within a greater context of interconnectedness; and provides them with tools to navigate and weave together these disparate parts.
No matter the technique, the journey back is always one of re-empowerment, of reclaiming our life and the wounded aspects of ourselves, and of re-engaging with the world. As we take this journey to heal our traumas, it is vitally important that we hold ourselves, like that bird, with tenderness, patience, compassion, and gentle encouragement. Whatever that overwhelm was or is, it feels HUGE! We have to allow ourselves to take small, slow ‘baby-steps’, as we transcend the trauma and come back to social engagement with others and peace within ourselves. Know that this is not only possible, but you are already on your way!
Exercise 1 – Pulsing Breath
In a relaxed seated position (on a floor cushion or in a chair) with your spine erect and not leaning against any support, slowly increase the depth of your breathing. Notice your shoulders raise with each In-Breath and fall with each Out-Breath. If possible breathe through your nose with your mouth closed and your tongue pressed gently to the roof of your mouth.
Gradually allow your breathing to become more accentuated. Breathe at a pace and rhythm that is comfortable to you. The breath can speed up and even become more syncopated/accented. Explore different speeds, rhythms and movements to pump blood into different areas. The shoulder girdle can move forward, rounding the chest; or back, opening the chest. And the motion can be up and down or forward and back. Do this exercise for 30-seconds to several minutes.
You may get light-headed from the increase in oxygen, don’t overdue it! End on a long, extended Out-Breath, completely emptying your lungs and hold for several seconds. Resume regular breathing when your body wants a breath. Take a moment to notice how you feel. What changed from before doing the exercise? You can repeat this sequence again. Remember to Play, and have fun with this as you reconnect to your body and its sensations.
REMEMBER: ALWAY LISTEN TO WHAT IS COMFORTABLE FOR YOUR BODY!
Polyvagal Theory Resources:
- Dana, Deb A., Anchored: How to Befriend Your Nervous System Using Polyvagal Theory (2022)
- Dana, Deb A., The Polyvagal Theory in Therapy: Engaging the Rhythm of Regulation (2018)
- Porges, Stephen W., The Pocket Guide to the Polyvagal Theory: The Transformative Power of Feeling Safe (2017)
- Rosenberg, Stanley, Accessing the Healing Power of the Vagus Nerve: Self-help Exercises for Anxiety, Depression, Trauma and Autism (2017)
- Also go to blogs Resourcing: Meeting Life’s Challenges
- Overwhelm: The Root Cause of All Disease – Parts 1 to 4
- Trauma & Bodywork Thesis
- Body-Mind-Spirit 1: Consciousness
- Suicide Prevention Hotline: 800-273-TALK (8255)
- National Suicide Prevention Lifeline
Disclaimer:
The information featured on this site is provided for information and education purposes only and is not intended to replace the advice of your doctor or health care provider on medical and/or health-related issues.
You should not use the information on this site for diagnosis or treatment of any health problem or as a substitute for medication or other treatment prescribed by your physician or health care provider.
Submit your review | |